On Episode 101 of Health in 2 Point 00, there are some scandals and competitors brewing in the health tech space! Jess and I discuss Outcome Health’s investigation and charge by the FBI for $1 billion in fraudulently obtained funds; Mint’s founder starting Vital, a new EHR company, to reinvent the overall EHR experience (even though I believe it is currently one of the toughest markets to enter into); Amazon launching Amazon Transcribe Medical which will be a tool medical professionals can use to dictate their notes and streamline them into EHR systems; and Wellframe raising $20 million to advance digital health management. If you are in Japan, catch me at Health 2.0 in Tokyo, Japan where they will be showcasing new health tech startups in the space or if you are in Vegas, go hang with Jess at the American Society of Hospital Pharmacies conference! Last but not least, Guidewell launched its Aging in Place Accelerator that is looking for startups in the senior health tech space (applications are due December 8th). — Matthew Holt
The post Health in 2 Point 00, Episode 101 | FBI Scandals, EHR Competitors, & Amazon appeared first on The Health Care Blog.
When Samuel Morse left his New Haven home to paint a portrait of the
Maquis du Lafayette in Washington DC, it was the last time he would see his
pregnant wife. Shortly after his arrival in Washington, his wife developed
complications during childbirth. A messenger took several days on horseback to
relay the message to Mr Morse. Because the trip back to New Haven took several
more, his wife had died by the time he arrived at their home. So moved was he by the tragedy of lost time
that he dedicated the majority of the rest of his life to make sure that this
would never happen to anyone again. His subsequent work on the telegraph and in
particular the mechanism of communication for the telegraph resulted in Morse
code – the first instantaneous messaging system in the world.
Mr Morse’s pain is not foreign to us in the 21st century. We feel the loss of new mothers so deeply that, when earlier this year new statistics on the rate of maternal death were released and suggested that American women died at three times the rate of other developed countries during child birth, doctors, patient advocates, and even Congress seemed willing to move heaven and earth to fix the problem. As someone who cares for expectant mothers at high risk for cardiovascular complications, I too was moved. But beyond the certainty of the headlines lay the nuance of the data, which seemed to tell a murkier story.
First at issue was the presentation of the data. Certainly, as a rate
per live births, it would seem that the United States lagged behind other OECD
countries – our maternal mortality rate was between 17.2 and 26.4 deaths per
100,000 live births, compared to 6.6 in the UK or 3.7 in Spain. But this
translated to approximately 700 maternal deaths per year across the United
States (among approximately 2.7 million annual births). While we would all agree
that one avoidable maternal death is one too many, the low incidence means that
small rates of error could have weighty implications on the reported results.
For instance, an error rate of 0.01% would put the United States in line with
other developed countries.
Surely, the error rate could not account for half the reported
deaths, right? Unfortunately, it is difficult to estimate how close to reality
the CDC reported data is, primarily because the main source data for maternal
mortality is a single question asked on the application for death certificates.
The question asks whether the deceased was pregnant at the time of death,
within 42 days of death, or in the 43 to 365 days prior to death. While
pregnancy at the time of death may be easy to assess, the latter two categories
are subject to significantly more error.
Just how much error is remarkably uncertain. One program called Review to Action attempted to ascertain this error rate by using Maternal Mortality Review committees to better understand the real causes of death among women who died around the time of the birth of their child. They looked at data from four states (Colorado (2008-12), Delaware (2009-14), Geogia (2012-13), and Ohio (2008-12)) to see if a deeper look at maternal deaths could uncover the true drivers of maternal mortality. Of the 650 deaths examined, 97 had no evidence of pregnancy in the year prior to death, a false positive rate of 15%. Among the remaining 553 deaths deemed “pregnancy associated” (death within one year of being pregnant), only 175 were thought to be pregnancy related, defined as “the death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy related complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy.” If this number was used to define maternal mortality, the rate would be 5.8/100,000 births, similar to other OECD countries.
Of course, this is an unfair comparison, because there is great
variation in how maternal mortality rates are calculated across the world. Moreover,
the rate of error in small numbers has as much likelihood of underreporting as
it does overreporting. But it does demonstrate a core problem in the
measurement of maternal mortality. Because the numbers are so small to begin
with, small errors have the risk of having significant effects on the results.
Even with uncertainty in the incidence, could we learn something
from those deaths confirmed to be pregnancy related? In cardiology circles,
there is great emphasis placed on the fact that the leading cause of death was
cardiovascular disease. If true, this could offer significant insight on how to
make an impact on reducing maternal deaths. But the devil is in the details,
and here the details suggested that in order to make cardiovascular disease the
leading cause of pregnancy-related death, we had to combine stroke, cardiomyopathy,
and “other CV conditions” which include a variety of conditions (including
congenital, ischemic, hypertensive and other heart diseases) (taken from MMWR
report on pregnancy related death). Though this broad grouping may make
epidemiologic sense, it makes less sense when attempting to build measures to
prevent death.
This is at the crux of the problem of the overemphasis on these statistics. They enable well-meaning people to create broad policies that have the potential for more harm than good. Take, for example, the administrator who boasted that he reduced the death rate to half the national average by getting automatic chest x-rays for all pregnant women with shortness of breath and automatic treatment for hypertension. At first blush it seems an impressive statistic. But even if they started at the national average, they would have reduced maternal deaths by 18. How many pregnant women received unnecessary chest radiation and medications to achieve that goal? The risks to casting wide nets to catch rare conditions are real and sometimes outweigh the benefit gained.
To understand where the balance of risks and
benefits are optimized, we must start with an earnest accounting of the data in
the public sphere. As currently reported
in both the medical and the lay media, the limitations of data derived from
small numbers are not discussed. Though messier than the headlines suggest, this
nuance offers the chance to shift focus to the actions that give clinicians,
patients, and caregivers the tools to really advocate for women at risk.
We also need to lower the barriers to expertise.
Cardiac obstetrics teams have become more common but are still not widespread. Most
programs offer great multidisciplinary care for patients with established risk,
but few offer virtual services to support the care of lower risk patients with
complex circumstances. Conditions like mild hypertension, edema, or even
palpitations are often benign conditions, but easily accessible expert support
for these circumstances could help identify signals of increased risk at times
and reassurance to the mother and her primary doctor at others. In the group I
work in, we have attempted to address this problem by creating a telemedicine
based consult system, so patients can be cared for by their own doctor with the
benefit of background support of a larger village of experts. Building virtual
support networks to broader populations offers the chance to create a safety
net without the risks of overtreatment seen with reflexive care algorithms. And
critically, patients can still be cared for by their own doctors, who they know
and trust.
We also need to rebuild the village of support networks
around new mothers. Many of the interventions that can reduce maternal risk
have to do with early detection, identification of conditions like post-partum
depression and unsafe home situations, and simpler things like offering new
moms time to engage in self-care (exercise, sleep, stress reduction, eating right).
While medical interventions seem to center on the detection of disease once
medical care is sought, broadening the frame of care and creating the
opportunity for peer based social support has the chance of helping all new
moms, not just those at highest risk.
Most importantly, though, we need to acknowledge the complexity of the issue of maternal mortality. Our solutions are not as singular as they were for Mr Morse, and accepting this will give us our best chance at success. For us, the answer is likely a series of incremental solutions, both small and large, working together to extinguish once and for all the tragedy of lost time.
Dr Ameya Kulkarni is the Chief of Cardiology in Northern Virginia at the Mid-Atlantic Permanente Medical Group.
The post Maternal Mortality – Separating Signal from Noise appeared first on The Health Care Blog.
Sean Duffy, CEO of Omada Health, proves why his company is one of those digital health startups everyone’s watching in the chronic condition management space. Never mind the buzz around their latest massive funding round or Livongo’s IPO, the real story here is Sean’s idea about building a “completely digital” care provider for folks with pre-diabetes, type II diabetes, hypertension, and mental health issues — or, at least that’s the goal for the next decade. What does a “full-stack view of supporting someone’s care look like? How do you get there? Tune in to find out about Omada’s proprietary tech-testing litmus test, “The Sean Duffy’s Mom Test,” and some good advice for other health tech startups about what it takes to win over clinicians with your tech.
Filmed at Health 2.0 in Santa Clara, California in September 2019.
Jessica DaMassa is the host of the WTF Health show & stars in Health in 2 Point 00 with Matthew Holt. Get a glimpse of the future of healthcare by meeting the people who are going to change it. Find more WTF Health interviews here or check out www.wtf.health.
The post Will Omada Health be Digital Health’s Next Big IPO? | Sean Duffy, Omada Health appeared first on The Health Care Blog.
There are only a few days remaining to apply for GuideWell’s 2020 Accelerator: Aging in Place! The program is seeking innovative, easy-to-use solutions that enable seniors to improve overall physical and emotional wellness, connect seniors to their communities, and increase the affordability and accessibility of health care for seniors that are economically challenged or cared for by a working family member.
10 health technology companies or innovators
will have the incredible opportunity to participate in an eight week
accelerator program that consists of a two-day kickoff boot camp, followed by
weekly mentoring sessions and a series of virtual workshops that focus on
challenges in the health care industry (e.g. customer acquisition, regulatory
compliance, etc.).The program begins January 23rd, 2020 and will culminate in a
curated Investor Matchmaking Showcase at GuideWell’s Innovation Center in
Orlando, FL., on March 9th, 2020.
Cohort
Company Criteria:
Eligible companies must meet GuideWell’s
minimum “Scale Up” requirements. A Scale Up is a growing technology startup
that has clear traction in its chosen marketplace. Traction can be demonstrated
by one or more of the following:
• A minimum of
$500,000 in revenues
• $500,000 in seed
capital raised
• Verifiable
(reference required) customer pilots
• Accelerating
product adoption (especially for consumer-focused solutions)
If you are an innovator with a next-generation solution, apply today! https://guidewellinnovation.com/guidewell-scale-up-accelerator/
Catalyst @ Health 2.0 (“Catalyst”) is the industry leader in digital health strategic partnering, hosting competitive innovation “challenge” events, as well as developing and implementing programs for piloting and commercializing novel healthcare technologies.
The post Applications for GuideWell’s Scale Up Accelerator Closing Soon! appeared first on The Health Care Blog.
Today on THCB Spotlights, Matthew interviews Todd Clardy who is the EVP of Marketing at Accolade. Accolade is a company well-known for being in employee/patient advocacy. They’ve created an advocacy model that focuses on creating an outstanding member experience and supporting patients through their whole journey, whether it’s an acute or chronic condition or helping people maintain their health and wellness. Where do Amazon, Google and Haven fit into this space? Find out how many people have got this and how Accolade will be expanding going forward.
The post THCB Spotlights: Todd Clardy, EVP Marketing at Accolade appeared first on The Health Care Blog.
At the end of the year my patients and I will start over. That is what changing EMRs does to us. I have mixed feelings about data migration, if it even happens.
I will move into a new virtual environment and my patients will take on slightly different appearances, maybe even alter their medical histories. Some will perhaps be asking me to edit diagnoses that have haunted them since we went from paper to computer records almost a decade ago.
With our first EMR, we scanned in a few things from patients’ paper records – sometimes only a few pages from years or decades of first handwritten and later typed notes. Much got lost, because we were doing something we never really had thought through, and we had to do it with a clock ticking: “Hurry, before the Federal incentives go away”. The Feds wanted EMRs because the vision was that more data would help research and population health and also reduce medical errors.
This time, another factor is pushing us forward: The EMR we have will no longer be supported after a certain date, and for an EMR that requires continuous tinkering in order to do basic tasks consistently, that is an untenable scenario. Only yesterday, I was suddenly unable to send prescriptions electronically and it took the national headquarter’s involvement to get me up and running again.
Our old EMR will become “read-only”, and who knows how much structured data will “migrate” from the old to the new system. And some information that should have been structured isn’t, because the old system’s search function was clunky enough that if we couldn’t find the exact word for a rare diagnosis in someone’s medical history, we would give up and choose the generic “neurologic disorder” and then free text the thing we might not even be spelling correctly. That still displayed intelligibly enough while the system was live, but will that migrate to the new system – who knows? Of course, there will be opportunities to correct old mistakes and omissions, as long as there is time…
The only way to view this inevitable transition is as an opportunity to undo old beginner mistakes, bad habits and workarounds. Having worked with two systems in my two clinics, I feel this is a bit like learning a new language or instrument; I know better what functionality I am looking for and will recognize it when I see it – just like a Spanish word I don’t know might look similar to a French word I do know for the same thing.
Wise from my positive experiences of screen sharing, I will bring patients along on this journey. I will be sitting next to each one with my laptop in front of us. I will invite them to update their history and increase the transparency of how I work, because there isn’t enough time in the day to keep the EMR invisible from my patient and then do all that work outside the appointment. Also, this is an era of increasing patient centeredness and I want to embrace that as much as I can.
I am determined to become as expert as possible with the new system so that I can document everything in real time in the visit and use more of my non-patient time in front of the screen to build templates and things like that.
In a way I feel a bit like many, many years ago when, as a student or budding writer, I opened a brand new notebook and put my pen to it for the first time. I loved fountain pens, crisp paper, leather bindings and the potential of all that clean, empty space.
Instead of feeling this EMR change will be a chore, I feel like a new school year or a new writing project is just about to begin.
Hans Duvefelt is a Swedish-born rural Family Physician in Maine. This post originally appeared on his blog, A Country Doctor Writes, here.
The post Changing EMR – Seamless Continuation, Dreaded Chore or Fresh Start? appeared first on The Health Care Blog.
If you’re used to health tech meetings filled with go-go entrepreneurs and the investors who love them, a conference of academic technology experts can be jarring.
Speakers repeatedly pointed to portions of the digital health superhighway that sorely need more concrete – in this case, concrete knowledge. One researcher even used the word “humility.”
The gathering was the annual symposium of the American Medical Informatics Association (AMIA). AMIA’s founders were pioneers. Witness the physician featured in a Wall Street Journal story detailing his use of “advanced machines [in] helping diagnose illness” – way back in 1959.
That history should provide a sobering perspective on the distinction between inevitable and imminent (a difference at least as important to investors as intellectuals), even on hot-button topics such as new data uses involving the electronic health record (EHR).
I’ve been one of the optimists. Earlier this year, my colleague Adrian Gropper and I wrote about pending federal regulations requiring providers to give patients access to their medical record in a format usable by mobile apps. This, we said, could “decisively disrupt medicine’s clinical and economic power structure.”
Indeed, the regulations provide “a base on which innovation can happen,” declared Elise Sweeney Anthony, executive director of the policy office of the Office of the National Coordinator for Health Information Policy, at one session.
But a base is only that. While Apple has already unveiled an app allowing people to see their health record on their iPhone, as yet there’s no “transformative business model” propelling hospitals to reach out to patients, said Julia Adler-Milstein, director of the Center for Clinical Informatics and Improvement Research at the University of California, San Francisco. Nor is there any indication from her research that many patients are interested.
“It’s still early days,” she added.
Similarly, Fitbit and Google announced their intent to combine patient-generated health data with clinical information in the EHR well before Fitbit agreed to Google’s $2.1 billion takeover bid. However, researchers studying the implementation requirements for this type of integration see far more than a bit that doesn’t yet fit.
One challenge for any app using patient-reported health data is standardizing symptom descriptions in a way patients will understand and yet still yields clinically useful results. Not to mention concerns about data validity. (See: “Want to cheat your Fitbit? Try a puppy or power drill.”)
“It’s appropriate to have humility,” said Robert S. Rudin, a senior information scientist at RAND. He added, in language virtually identical to Adler-Milstein’s, “This is still early days.”
A major symposium theme was “proactive health care,” or using patients’ health data to prevent or ameliorate illness. One focus was screening patients for the hodgepodge of food, housing and other non-medical issues known as “social determinants of health” (SDOH). The process seems straightforward: ask patients about their circumstances, load the answers into a database and apply algorithmic analysis. Out pops guidance for addressing the social and economic factors that account for 40 percent of each individual’s health outcomes, compared to the 20 percent from clinic care.
Once again, however, important elements remain unresolved. Are the questions valid? Can one trust patients’ recall? Does the whole process even improve outcomes? One recent analysis even warned that some “efforts could worsen health and widen health inequities.”
“I’m not sure we’ve worked out these basic issues,” said Jessica Ancker, an associate professor in Weill Cornell Medicine’s division of health informatics
Of course, academics have their biases (“Further research is needed”), just as entrepreneurs have theirs (“It’s not a bug, it’s a feature”). Not to mention humorist James Boren’s memorable advice to bureaucrats. As I’ve previously suggested, assembling a group of regulators, innovators and evidence-makers to talk candidly with each other might significantly accelerate digital health innovation.
For example, the Google and Ascension Health execs who launched the much-criticized “Project Nightingale”could have have benefited from a blunt warning about big data from Lamiece Hassan, a health data research fellow at England’s University of Manchester.
“People have expectations about what information to share and how that information flows,” she said. “Just because the data are accessible doesn’t make it ethical.”
Michael L. Millenson is president of Health Quality Advisors LLC and adjunct associate professor of medicine at Northwestern University Feinberg School of Medicine. This article originally appeared on Forbes here.
The post Concrete Problems: Experts Caution on Construction of Digital Health Superhighway appeared first on The Health Care Blog.
Quil Health CEO, Carina Edwards, tells us what’s happening at the digital health startup born from the partnership between Comcast NBCUniversal and Independence Blue Cross. The new “baby” is just about a year old. How’s it fairing? And how involved are the “parents”? Carina talks about the company’s patient engagement platform that connects via phone, web, and cable TV. That means 30 million Comcast subscribers can sync their TV with their Quil app and literally ‘watch’ their care plan along with their Nightly News. Will Al Roker be making another appearance on Quil soon? This, and all the important questions about their business model and client base are answered here!
Filmed at the HIMSS Health 2.0 Conference in Santa Clara, CA in September 2019.
Jessica DaMassa is the host of the WTF Health show & stars in Health in 2 Point 00 with Matthew Holt. Get a glimpse of the future of healthcare by meeting the people who are going to change it. Find more WTF Health interviews here or check out www.wtf.health.
The post Now 30M Comcast Members Can Sync their Care Plan with their TV | Carina Edwards, CEO Quil Health appeared first on The Health Care Blog.
No one likes getting bills. But there is something that stinks particularly spectacularly about bills for healthcare that arrive despite carrying health insurance. Patients pay frequently expensive monthly premiums with the expectation that their insurance company will be there for them when illness befalls them.
But the problem being experienced by an
increasing number of patients is going to a covered (in-network) facility for
medical care, and being seen by an out-of-network physician. This happens because
not all physicians working in hospitals serve the same master, and thus may not
all have agreed to the in-network rate offered by an insurance company.
This is a common occurrence in medicine.
At any given time, your local tax exempt non-profit hospital is out of network
of some low paying Medicaid plan or the other.
In this complex dance involving patients, insurers and doctors, Patients want their medical bills paid through premiums that they hope to be as low as possible, Insurers seek to pay out as little of the premium dollars collected as possible, and Doctors want to be paid a wage they feel is commensurate to their training and accumulated debt.
Insurers act as proxies for patients when
negotiating with the people that actually deliver healthcare – doctors.
Largely, the system works to funnel patients to ‘covered’ doctors and
hospitals. Patients that walk into an uncovered facility are quickly
redirected. But breakdowns happen during emergencies.
There are no choices to make for patients
arriving unconscious or in distress to an emergency room. It suddenly becomes
very possible to be seen by an out of network physician, and depending on the
fine print of the insurance plans selected some or none of these charges may be
covered.
Physicians that typically prefer banal
chants of “health is care for all” and avoid deep dives into policies
that determine physician reimbursement may want to pay attention to the debate
because it provides a clear picture of the forces currently trying to shape the
conversation about how to value physicians. The news is not good.
Practically speaking, no physician wants the hassle of being out of network. Ethically, few physicians have the stomach for bankrupting patients, and attempting to collect from the uninsured isn’t a desirable brand to cultivate. For those patients left with a balance, its actually illegal on the part of physicians to not attempt to collect. On the inevitable non-receipt of the balance, steep discounts or a write-off follows. So despite the heated rhetoric surrounding physicians ‘fleecing’ patients, the amount of real dollars collected from patients is never mentioned. While this number is hard to ascertain, a good proxy may be medical bankruptcies, which is a relatively rare event. So the amount of smoke that has been generated from, what in absolute terms, is a small fire has little do with patients and everything to do with how we figure out what to pay physicians.
The traditional leverage physicians have employed against insurers is the ability to not accept rates offered by payers. This isn’t unusual – its fundamental to every negotiation between two parties where the laborer isn’t conscripted. A mango seller has a price below which he won’t sell mangos. The negotiation would go much differently if the mango seller was compelled to sell his mangos at some price. The problem for insurers is that the pressure from patients to have in-network doctors is intense. Patients pay steep monthly premiums so they won’t get large, potentially bankrupting health care bills when they need medical care. And so the ability of physicians to not accept a proffered rate is fundamental to the negotiation between insurer and physician. The threat of a doctor being out of network raises the in-network rates. The threat of not getting a mango belie a certain price raises the price of the mango. Not complicated.
Further more, physicians that deliver services during emergencies – anesthesiologists, ER physicians, orthopedic trauma, neurosurgery – have greater leverage than physicians who don’t deliver emergency care. Insurers are far more effective at negotiating with primary care physicians because a primary care physician who chooses not to accept the contract of a certain insurer effectively shuts themselves out of that network. Insurers have no such luck directing patients in times of emergencies. The demand for services in this context is ‘inelastic’, giving physicians significant latitude in negotiating contracts with insurers. This is a giant thorn in the side of insurance companies that complain high medical premiums are a direct result of the high prices they must pay for these services.
‘High’, of course, is a relative term. They think of the rates they pay relative to the rates Medicare pays. Medicare enjoys one of a kind leverage because it is a legislatively created behemoth consolidating the buying power of the entire over 65 population under a government administered and enforced program. That leverage means Medicare rates are significantly lower than private rates, and specialties with greater inelastic demand are able to extract significant multiples of Medicare rates.
Insurance companies would like nothing
more than legislative help that would limit the amount they have to pay
physicians. Their ally in this fight is the simple fact that health care isn’t
quite like selling mangoes. In the healthcare marketplace, vulnerable patients
arrive in emergency departments in extremis with little ability to make choices,
and so many argue this is the very place the government needs to protect
hapless citizens.
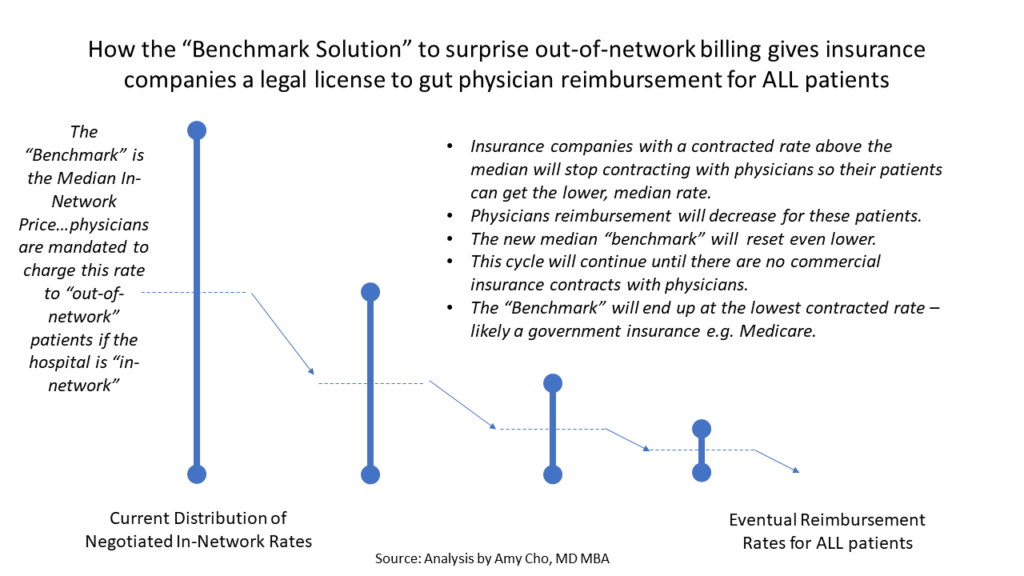
The solutions that comes from health
policy/economists is also endorsed by the Senate Health, Education, Labor and
Pensions committee (HELP). This bipartisan group supports federally benchmarked
caps on rates that can be charged that are pegged to the median (50%)
in-network rate for an area. So if a patient happens to be seen by a physician
that is out of network, the insurer would pay the median in-network rate in the
area. But in this plan, there would be no incentive going forward for insurers
who contract at higher than the median in-network rates to stay in-network.
What would be the point? Just drop the contract, since the out of network rate
gets you 50% of the area in-network rates. This creates a race to the bottom
that effects reimbursement rates for all patients.
Figure courtesy of @amychomd
Physicians in practice and in congress
favor a different approach to get patients out of the line of fire: Independent
Dispute Resolution (IDR). The IDR, implemented in New York City in 2015, seeks
to take patients out of the middle by sending disputes between providers and
insurance to binding arbitration. Generally, the effect is that providers and
insurers settle disputes between themselves before a third party gets involved.
The desire to avoid potential third party arbitration also has the effect of
increasing in-network rates. This isn’t theory. The New York legislation
increased in-network provider participation, saved patients money, and lowered
in-network physician rates.
Interestingly, the health policy
community has taken the tack of rejecting the physician endorsed solution, and
accusing supporters in the provider community as greedy shills interested in
profits over patients. A frequently raised point is the fact that some Private
Equity firms own ER groups and are lobbying for IDR and against median
benchmarking. Apparently, any policy that would result in Private Equity
profiting is a bridge too far for the policy community. It goes unmentioned
that in the battle between insurers and doctors, the health policy community
places itself squarely on the side of health insurance company profits.
There is also remarkably little
appreciation for the second order effects of decreasing reimbursement to
physicians expected to be ready for emergencies. The vessel that bursts in your
brain requires a team acting quickly to recognize and treat this emergency.
Will neurosurgeons, anesthesiologists , and emergency medicine physicians of
quality be available at 2 am? Neurosurgeons are likely to choose to avoid being
on call, and recommend transferring patients to facilities with the scale and
infrastructure to keep Neurosurgeons on call for emergencies. Transfers to quaternary
care facilities take time. Time is brain. The amount of brain damage is the
difference between slight weakness of that right hand grip while drinking a
glass of wine at home or a dense paralysis of the entire right half of your
body that translates to a nursing home and a feeding tube. The potential downsides of policy that
reduces reimbursement to a highly specialized group and thus could reduce
access are not small, but seem to be underappreciated by policy ‘experts’
bending the ear of members of Congress.
Policy experts are experts not because
they have any experience trying to manage and run a physician practice, but
because they are lords of the empiricism found in the peer reviewed literature
of the day. For some reason this puts
them on a level playing field with the people who run practices and have to
meet payroll every 2 weeks. Its certainly possible the process of running a
business is entirely too narrow a field of view, but its unclear that the
policy experts field of view is more enlightening.
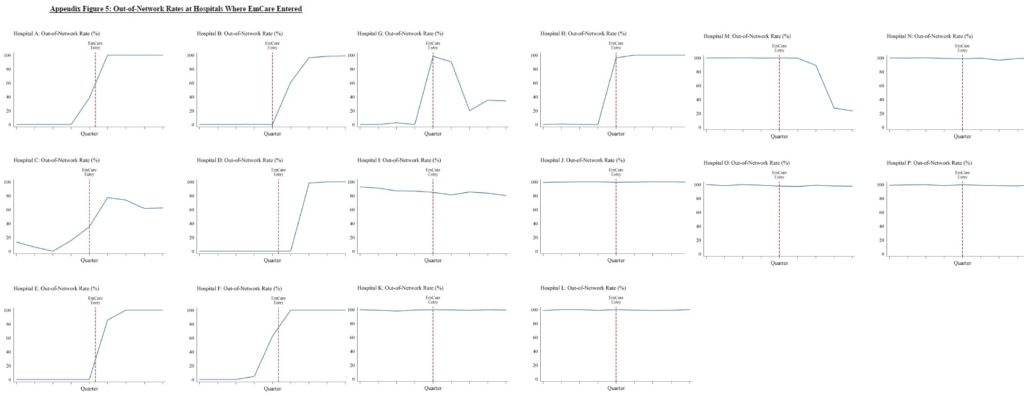
Zach Cooper at Yale has done a lot of work in this space, and one of his papers that is cited often is derived from claims data provided by a large private insurer. The general hypothesis of the study is that large profit hungry private firms that own ER practices flung across the nation engage in predatory activity once they acquire a local ER group. This ultimately raises costs to the patient, and thus damages societal welfare as a whole. Using the company websites of the private firms, the researchers were able to divine that the two companies (TeamHealth and EMcare) were involved in a whopping 9% of their national sample. In order to understand how the entry of these firms may impact medical charges and reimbursement, the investigators found a total of 26 hospitals the firms initiated contracts with in the time frame studied.
The authors divine many thing from the
raw data. To support the claim that arrival of the private groups may have
increased out of network rates to fleece patients and improve their leverage
for in-network rates the authors examine the data and conclude: “In Panel
A of Figure 3, the raw data show a clear increase in out-of-network billing
rates at hospitals immediately after EmCare entered.” The strange thing, however, is that the raw
data of the 16 hospitals there was data on that looked at OON rates after EM
health enters a market, shows a clear temporal association of rates rising
after EM health arrived in only 2 cases. In 4 hospitals, OON rates started to
rise before EM health entered, and in the remaining cases, OON rates were
either unchanged, or were seen to decrease.
The authors proceed to firmer footing
when they discuss the charges billed, because the insurer they are working with
has been nice enough to provide this information for every patient they
received a charge for. They find that the entry of EMcare increases charges by
$556.84 (96%). They note that some of this increase occurred because the
intensity of coding that reflects how sick the patient is increased significantly
soon after EMcare enters. The implication, of course, is made that this
upcoding is improper, yet no support is provided for that assertion. It is just
as plausible that physicians were
undercoding the severity of patients prior to EMcare entering the market – this
narrative defying possibility goes unmentioned.
The absolute amounts being discussed also
bears attention. The OON payments that
were paid by insurers after EMcare entered the market increased by $402.67.
Patient cost sharing payments increased by $45. Now it is possible that
patients may have balances beyond these paid charges, but even this amount
comes to $195. These averages paid here exclude ~ 217,000 claims where insurers
paid nothing because of a claim denial.
These numbers aren’t zero, but for emergency medical care, these numbers
($195+ $45) are still far south of the average apple watch.
The most vulnerable patients of course,
don’t have health insurance, and aren’t buying apple watches. For this group, the total potential liability
could range from $578 to $1135. It
isn’t known what is actually collected from this group of patients as the
administrative costs of trying to collect in this population are not small, and
there is most certainly a reputational cost to bear in the community for
generating these bills.
The underlying assumption that runs
through the paper is that the price being paid for these services is too high
because patients are unable to shop for care in an emergency. But this ignores the fact that in our
current system, its the insurance company that acts as an agent for the
patient. They are well aware when they
sign patients up for a health care plan that an out-of-network may happen. So while much of the focus in this debate is
on the bill generating providers, one wonders how it came to be that that
insurance plans are allowed to sell plans to patients that don’t offer any out
of network coverage. Should a facility
be considered in-network if physicians that work at the facility are out of
network? Shouldn’t patients be informed of this by their insurance company? The
insurance company is fully aware of the consequences – so why is the bill that
passes through to patients a surprise? The only party with foreknowledge of
what may happen is the insurance company.
They have every ability to shop on the marketplace, and it is their
failure to secure a contract and then communicate this to their customers that
results in ‘surprise’ bills.
In order to buttress the idea of ‘high’
cost, the paper attempts to use reference Medicare payments. Its noted that Internists are paid 158% of
Medicare rates, orthopedists 266% of Medicare rates while the rates paid to the
2 ER firms in the paper are 364% and 536% of Medicare rates. It only serves passing mention that the
average amounts paid exclude 217,000 claims where nothing was paid because the claim was denied. There is also no mention made of the
difference between elective care provided by orthopedists and internists versus
the almost entirely emergent care provided by ER physicians that is delivered
without consideration of the patients ability to pay. ER physicians are legally (because of a law
called EMTALA) and ethically bound to take care of patients who arrive in the
ER in distress. This means they shoulder
a far heavier responsibility for uninsured care than almost any other
specialty. Most physicians who deliver
care in the outpatient setting require a payment arrangement be made prior to
seeing a patient. The ER physician has
no such recourse. Not mentioning this
when discussing rates paid to ER physicians, and other physicians delivering
care in emergencies is a feat of obfuscation and deception.
The researchers and other commentariat
from the policy community also seem to fail at understanding the motivations of
doctors in the current system. I can think of no physicians that want patients
getting these bills. In the current
third party payer system, opacity is the physicians friend. Given the reputational cost, and the
administrative cost of trying to collect these bills, physicians more so than
policy wonks are highly motivated for a solution that takes patients out of the
mix and generally endorse the previously mentioned third party arbitration
system.
This is reluctantly analyzed by Cooper
et. al., as well. Implemented in New
York in 2014, the study finds that the OON rate went from 20% in 2013 to 6% in
2015. Unimpressed, the authors dismiss
the solution as being “administratively complex and potentially
costly” because it requires patients to know about, and fill out a one
page form if they were to receive a bill.
This ‘analysis’ misses the fundamental point that IDR results in a huge
drop in the chance these bills are being sent to patients, or that most
disputes are resolved without even involving the IDR.
One is struck by the hubris of the
inevitable conclusions the researchers arrive at based on data provided from
one insurer and an analysis of 2 firms. As noted previously, the raw data
consists of a small handful of hospitals from this already small sample, and
doesn’t even tightly demonstrate the relationship of price to firm entry. Even
if we assume prices rise, the conclusion that consolidation raises prices.
Water, I’m told, is also wet. No data is provided on changes to the local
marketplaces in this small sample during the time studied. Profit seeking is
certainly one plausible explanation, but its also just as possible that a
greater proportion of underinsured or poorly insured patients arriving in the
ER during the same time was responsible for raised rates. Apparently the policy
memory is amnestic to The Dartmouth institute that changed the landscape of
healthcare policy with its reports of regional variation Medicare spending. The
small problem was that this dataset didn’t take into account private insurance
spending. Subsequent publication of data from the economists the insurance
industry uses (Cooper et. al) invalidated the Dartmouth data. Context matters.
So this battle has little to do with
patients. The rejection of the IDR in
favor of an untested proposal physicians don’t endorse is part of an
ideological battle waged by a group of folks that have decided health care is
too expensive (it is) and that physicians need to be devalued to create a
better system. Data to support this
ideology conveniently comes from those with an outsize interest in paying less
for physician labor: the insurance industry that pays for healthcare in our
current system. Given that the only data
the insurance companies really have is the amount that they pay for services
rendered, it should perhaps come as little surprise the conclusions draw from
this data is as weak as it. Importantly, this data has little bearing on what
the right price for these services are, what the best mechanism to get the
right price is, or what the downsides of untried, untested policies are.
There is a real argument worth having
about health care prices and how they can be lowered. A number of regulatory
straitjackets harm competition and creates a landscape of large players that
have kept prices high. Sitting inside the guts of the healthcare system, it is
easy to see rent seekers in every health care sector that proliferate.
Physicians aren’t entirely blameless, and a better more efficient may very well
see many physicians making less, but it would be wise to act more like the
skilled surgeon rather than the butcher to avoid killing the patient.
Anish Koka is a cardiologist in practice in Philadelphia.
The post Guerilla Billing – Missing the Gorilla in the Midst appeared first on The Health Care Blog.
Today on THCB Spotlights, Matthew speaks with Jeremy Orr, CEO of Medial EarlySign. Medial EarlySign does complex algorithmic detection of serious diseases, working on early detection of cancer and the progression of chronic disease such as diabetes. Tune in to hear more about this AI/ML company that has been working on their algorithms since before many had even heard about machine learning, what they’ve been doing with Kaiser Permanente and Geisinger, and where they are going next.
Filmed at the HLTH Conference in Las Vegas, October 2019.
The post THCB Spotlights: Jeremy Orr, CEO of Medial EarlySign appeared first on The Health Care Blog.